As the saying goes, "There are routine surgeries, but there is no routine anesthesia." Taking a universal approach to anesthesia using a cookbook protocol can lead to dangerous situations.
Knowing how to recognize risk and respond appropriately can greatly decrease the likelihood of anesthesia-related complications.
How to decrease pre-op risks
The preoperative period is a critical time to identify any potential risk and take precautionary measures to reduce or eliminate it.
Fasting and withholding water are commonly done the night before surgery; however, this may not be appropriate for all patients. A blanket statement such as "No food or water after 8 p.m." or "No food or water after midnight" is not considered ideal.
Withholding food prior to anesthesia is recommended in most patients to lessen the risk of vomiting and aspiration. Juvenile patients and diabetic pets on insulin, however, can become hypoglycemic after so many hours of fasting. These patient-specific considerations need to be taken into account, which means "routine" pre-op protocols must be amended.
Withholding water can lead to mild dehydration in a healthy patient and more severe dehydration in geriatric or renal-compromised pets. Adequate hydration is key to having a successful anesthesia and surgery. Most surgeons allow water access until the morning of surgery.
Intravenous fluid should be given prior to anesthesia in dehydrated or renal-insufficient patients to correct electrolyte imbalances and other metabolic abnormalities, such as uremia, hypercalcemia, hyperkalemia, etc.
The patient's history should be reviewed for any potential risk factors that may not be detected on physical exam. Recording anesthetic complications or an adverse reaction to a particular drug or protocol is helpful for future anesthetic episodes.
A thorough physical exam and blood work should be performed before any anesthesia. Of course, blood work should then be reviewed and analyzed critically, rather than merely being added to the medical record.
Brachycephalic, cardiac, and dyspneic patients can be pre-oxygenated before induction and intubation to reduce the risk of hypoxemia. This is assuming pre-oxygenation doesn't cause stress in the patient, which would defeat the purpose.
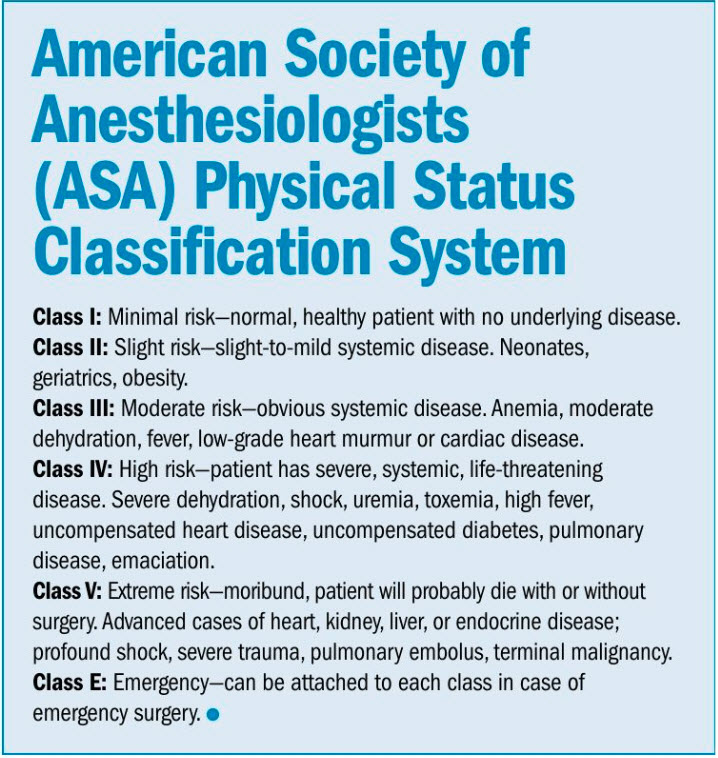
Patients with a physical status of "3" or greater on the American Society of Anesthesiologists (ASA) classification system (see sidebar) have a systemic disease that may increase their risk of anesthesia-related morbidity and mortality.
Faulty or malfunctioning anesthesia machines and equipment, as well as inexperienced staff, can further increase the anesthetic risk. This is the reason why an anesthesia machine should be checked thoroughly (including for leaks) at the beginning of each day, if not before every surgery. Anesthetic equipment also should be inspected yearly by a professional.
Simple precautions include turning the oxygen on, opening the pop-off valve, and ensuring there is enough anesthetic gas in the vaporizer. Also verify small endotracheal tubes are entirely clean inside and free of debris from previous patients to avoid causing an obstruction of the tube.
How to decrease intra-op risks
 Risks that were not properly identified or addressed in pre-op can quickly worsen during the intra-op phase. The procedure's type and involvement play a role in anesthesia risk. Those that are more complex or have higher organ involvement pose an increased risk for morbidity and mortality.
Risks that were not properly identified or addressed in pre-op can quickly worsen during the intra-op phase. The procedure's type and involvement play a role in anesthesia risk. Those that are more complex or have higher organ involvement pose an increased risk for morbidity and mortality.
Likewise, the longer the anesthesia, the higher the incidence of morbidity or mortality. Compromised, geriatric, and juvenile patients are at an increased risk due to their limited ability to appropriately compensate for stressors such as anesthesia. Emergency or trauma patients also are at an increased risk for anesthetic-related complications intra-op because they may not
have been adequately stabilized prior to anesthesia.
Three classic dilemmas are patients who are actively bleeding, those who have an acute diaphragmatic hernia, and those who have gastric dilatation-volvulus (GDV). Should they be stabilized or should they go straight to surgery? The answer is not as obvious as it seems.
Improper monitoring or lack of a timely response to trending changes in vital signs also can lead to anesthetic-related death. Continuous monitoring of anesthetic depth, blood pressure, CO2 levels, and multiple other parameters can make the surgical team aware of an anesthetic complication. This is the reason why documenting vital signs is so critical. Without a written record, how can you detect a trend?
Loud music, distractions, and interruptions in the OR also can increase complications because the surgical team may not be fully focused on the patient. Relying exclusively on electronic monitoring equipment can elevate the risk as well. Don't trust machines blindly. Trust your senses (eyes, sight, touch, even smell) and with experience, your gut, to anticipate complications.
If patients under anesthesia have low blood pressure, they could have compromised blood flow to vital organs such as the kidneys. A patient with renal compromise prior to anesthesia can have a higher risk of anesthetic complications if their blood pressure is not properly monitored and regulated.
Hypoventilation often occurs in anesthetized patients, especially those who are overweight and obese (obesity hypoventilation syndrome, a.k.a. Pickwickian syndrome). Monitoring CO2 is a very sensitive indicator of proper ventilation. Relying solely on O2 monitoring can be very misleading.
Decreasing post-op risks
Contrary to what most pet owners and even team members believe, the majority of deaths don't occur during anesthesia, but rather during recovery.* This is in part due to made-up rules that seem to be practice-dependent. The "two-swallow rule" and the "three-swallow rule" before extubation are dangerous at best.
The proper time to extubate is patient-dependent—there is no universal truth or magic number. In addition, extubated patients should be continuously monitored just as if they were still under anesthesia. Heart rate, respiratory rate, oxygenation, and temperature are some of the vitals that should still be checked until they have returned to normal or until the patient is alert, sternal, and/or moving around enough.
Hypothermia, hypotension, and decreased respiratory rate can lead to prolonged recovery time, which can increase the risk of post-op anesthesia complications. Extubating prematurely, deflating the cuff of the endotracheal tube too soon, failure to keep the head elevated, and lack of monitoring can lead to regurgitation, followed by aspiration pneumonia.
With thorough presurgical exams, ASA scoring, individualized anesthesia protocols, proper monitoring, as well as an experienced team, you can reduce the risk of anesthetic-related complications.
Phil Zeltzman, DVM, DACVS, CVJ, Fear Free Certified, is a board-certified veterinary surgeon and author. His traveling surgery practice takes him all over Eastern Pennsylvania and Western New Jersey. You can visit his websites at www.DrPhilZeltzman.com and www.VeterinariansInParadise.com. Kat Christman, a certified veterinary technician in Effort, Pa., contributed to this article.
References
* DC Brodbelt. "The Confidential Enquiry into Perioperative Small Animal Fatalities." 2006 thesis.